Partial Knee Replacement
KNEE PROBLEMS
SURGICAL PROCEDURES
Partial knee replacement or Unicondylar Knee Replacement (UKR) has
experienced a resurgence of interest with the introduction of minimally
invasive surgery. Numerous studies, including the Swedish Registry,
have demonstrated 90% or greater 10-year survival rates with unicompartmental
knee replacement systems. Unfortunately, survival rates beyond 10 years
have proved disappointing, falling to the 80% range. UKR has the disadvantage
that the medium and long-term revision rates are generally higher than
for TKR. UKR are therefore considered by many to be "pre-total
knee replacements", and are only expected to last for a relatively
short period.
However, twenty years of experience has led to a better understanding
of the optimal design features for unicompartmental replacement. The
newest implant systems for unicondylar arthroplasty provide both implants
and instruments that are designed specifically for minimally invasive
surgery. Medial unicompartmental knee replacement has many advantages
over total knee replacement (TKR). As all the undamaged structures of
the joint, in particular the cruciate ligaments, are preserved, knee
function can be restored to nearly normal. After UKR the range of movement
is better than after TKR, the knee feels more natural and pain relief
is as good or better. In terms of morbidity, operative blood loss is
minimal and transfusion is usually unnecessary, complications are less
frequent and less serious and recovery is generally quicker.
 |
 |
|
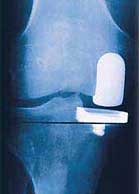
DePuy PFC Sigma unicompartmental
knee implants |
The main indication for unicondylar knee replacement is medial compartment
osteoarthritis. The anterior cruciate ligament should be functionally
intact. Fixed flexion deformity should be less than 15°. Varus deformity
should be correctable and there should be full thickness cartilage in
the lateral compartment. Knee X-rays, taken while standing, must show
complete loss of joint cartilage in the medial compartment. Lateral
unicompartmental replacement is still controversial, although several
surgeons claim good mid- to long-term outcomes.
Unicomparmental replacement appears to offer an early alternative to
osteotomy or tricompartmental arthroplasty in elderly patients with
unicompartmental arthritis. Compared to high tibial osteotomy, there
is a higher initial success rate and fewer complications. Compared to
tricompartmental arthroplasty, there tends to be a better functional
outcome with a faster recovery and improved function. With appropriate
patient selection, new generation of implant design, and minimally invasive
operative techniques, unicompartmental knee arthroplasty should assume
its proper role in the knee surgeon's armamentarium. High tibial osteotomy
should still be used as an alternative procedure in the young, heavy,
active individual.
ConforMIS Personalised Knee Implants
We are pleased to announce that we will start using ConforMIS iUni patient specific knee implants from September 2014. We introduced this new technology to the Grosvenor Hospital Chester in 2013. After almost two years of preparations, regulatory and clinical negotiations with healthcare insurers and Nuffield Health, imaging and theatre staff training we are ready to go! We will also start with ConforMIS iUni registry clinical study and will collect clinical and outcome data for each patient.
ConforMIS team has developed the only personalized knee resurfacing implants available today, designed to conform precisely to individual patient's unique anatomy. Using a proprietary technology called iFit (the "i" stands for individualized), ConforMIS creates implants which are made specifically for each patient. Personalized implants offer unique advantages versus traditional knee replacement options: superior fit matched to individual size and shape, natural, anatomic feel and alignment, significant bone preservation, less traumatic procedure and potentially faster recovery. For many patients, especially those who suffer from earlier stages of osteoarthritis, ConforMIS offers a range of implants that may provide a less invasive and less traumatic option than traditional knee replacement.


ConforMIS iUni Personalised Knee Implants
The iFit Image-to-Implant process uses CT imaging data to create personalized devices designed to achieve precise fit, preserve bone and cartilage, and minimize surgical trauma. This process begins when the patient receives a diagnostic CT scan. After the scan, the centre sends the data to ConforMIS via CD or secure internet file transfer. Using iFit technology, ConforMIS generates a 3D model of the patient's knee and then map the anatomy of the patient's joint. This technology creates an implant that is precisely matched to the patient's surface contours and anatomy.
Further Information:
- The Knee Society: Unicompartmental Knee Replacement.
- For more information on partial knee replacements, see DePuy Preservation website.
Page last updated on 8 June 2014
Site last updated on: 28 March 2014
|
 Disclaimer: This website is a source of information
and education resource for health professionals and individuals
with knee problems. Neither Chester Knee Clinic nor Vladimir Bobic
make any warranties or guarantees that the information contained
herein is accurate or complete, and are not responsible for
any errors or omissions therein, or for the results obtained from
the use of such information. Users of this information are encouraged
to confirm the accuracy and applicability thereof with other sources.
Not all knee conditions and treatment modalities are described
on this website. The opinions and methods of diagnosis and treatment
change inevitably and rapidly as new information becomes available,
and therefore the information in this website does not necessarily
represent the most current thoughts or methods. The content of
this website is provided for information only and is not intended
to be used for diagnosis or treatment or as a substitute for consultation
with your own doctor or a specialist. Email
addresses supplied are provided for basic enquiries and should
not be used for urgent or emergency requests, treatment of any
knee injuries or conditions or to transmit confidential or medical
information. If you have sustained a knee injury or have a medical condition,
you should promptly seek appropriate medical advice from your local
doctor. Any opinions or information,
unless otherwise stated, are those of Vladimir Bobic, and in no
way claim to represent the views of any other medical professionals
or institutions, including Nuffield Health and Spire Hospitals. Chester
Knee Clinic will not be liable for any direct, indirect,
consequential, special, exemplary, or other damages, loss or injury
to persons which may occur by the user's reliance on any statements,
information or advice contained in this website. Chester Knee Clinic is
not responsible for the content of external websites.
Disclaimer: This website is a source of information
and education resource for health professionals and individuals
with knee problems. Neither Chester Knee Clinic nor Vladimir Bobic
make any warranties or guarantees that the information contained
herein is accurate or complete, and are not responsible for
any errors or omissions therein, or for the results obtained from
the use of such information. Users of this information are encouraged
to confirm the accuracy and applicability thereof with other sources.
Not all knee conditions and treatment modalities are described
on this website. The opinions and methods of diagnosis and treatment
change inevitably and rapidly as new information becomes available,
and therefore the information in this website does not necessarily
represent the most current thoughts or methods. The content of
this website is provided for information only and is not intended
to be used for diagnosis or treatment or as a substitute for consultation
with your own doctor or a specialist. Email
addresses supplied are provided for basic enquiries and should
not be used for urgent or emergency requests, treatment of any
knee injuries or conditions or to transmit confidential or medical
information. If you have sustained a knee injury or have a medical condition,
you should promptly seek appropriate medical advice from your local
doctor. Any opinions or information,
unless otherwise stated, are those of Vladimir Bobic, and in no
way claim to represent the views of any other medical professionals
or institutions, including Nuffield Health and Spire Hospitals. Chester
Knee Clinic will not be liable for any direct, indirect,
consequential, special, exemplary, or other damages, loss or injury
to persons which may occur by the user's reliance on any statements,
information or advice contained in this website. Chester Knee Clinic is
not responsible for the content of external websites.