Knee Problems
KNEE PROBLEMS
SURGICAL PROCEDURES
See Also:
Introduction
The knee joint is a very complex structure that is vulnerable to injury in practically all activities. As fitness and sports activities are integral parts of our lives, injuries to the knee occur at alarming rate in all age groups. The knee is injured more frequently than any other joint in the body, but fortunately many knee problems do not require surgical treatment. Some knee problems are not injury related - generalised spontaneous aching and swelling usually suggest a degenerative process or arthritis.
Quite often it is difficult to establish the correct diagnosis soon enough and to treat the problem adequately. Over the past decade, the diagnosis and management of knee disorders have been improved significantly. Early diagnosis, both clinically and with Magnetic Resonance Imaging (MRI), better understanding of knee biomechanics, and the importance of preserving menisci, articulating surfaces and joint stability have greatly improved our ability to preserve and extend knee function.
The types of knee injuries very greatly - ranging from simple muscle strains, contusions and bruises to severe injuries of ligaments and articulating surfaces. Serious damage to the knee joint can increase the risk of accelerated wear and tear (post-traumatic arthritis, or more correctly arthrosis) and long-term disability. Some sports like football and squash are associated with a high incidence of meniscal, chondral and ligament injuries and consequent mechanical problems. Rapid effusion following sudden deceleration and twisting injury, usually suggests an anterior cruciate ligament tear. The meniscus is usually torn with a weight-bearing twisting movement, which is followed by a sharp pain and mechanical problems like giving way, catching and locking. For more specific information on meniscal, ligament, cartilage and other injuries and disorders please see our separate pages on the right hand side.
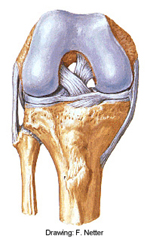
Basic Knee Anatomy
The knee consists of two joints made from three bones: tibia, femur
and patella. The tibio-femoral joint has medial and lateral compartments.
The medial and lateral femoral condyles articulate with the medial and
lateral tibial plateaus. The patella covers the front of the knee. The
patello-femoral joint is the articulation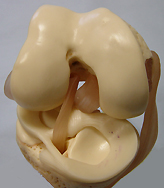 of the patella with the femoral
trochlea. All joint surfaces are covered with hyaline articular cartilage.
of the patella with the femoral
trochlea. All joint surfaces are covered with hyaline articular cartilage.
The quadriceps mechanism proximal to the patella consists of the vastus lateralis, rectus femoris, vastus intermedius and vastus medialis. The most distal and medial part of the vastus medialis is the vastus medialis obliquus. The quadriceps mechanism is continuous with the medial and lateral retinacula, which attach to and course along either side of the patella before inserting into the tibia. The quadriceps tendon attaches superiorly, and the band-like patellar tendon extends inferiorly towards the tibial tubercle. The prepatellar bursa and the superficial infrapatellar bursa allow the overlaying skin to move easily over the deeper structures.
The four major ligaments involved in knee stability are the medial collateral ligament (MCL), lateral collateral ligament (LCL), anterior crucuate ligament (ACL), and posterior cruciate ligament (PCL). Although medial stability is provided mainly by the MCL, the lilotibial band (ITB), lateral capsule, politeus tendon, LCL, biceps femoris, and lateral head of the gastrocnemius muscle all contribute to lateral stability. The tibial surface is partially covered by the medial and lateral menisci, which attach to the tibia by the coronary ligaments.
- YouTube Knee Anatomy Video Tour
- YouTube Knee Ligament Anatomy Animation, Bertram Zarins, M.D.
Basic Knee Biomechanics
The cruciate ligaments enable the knee to both roll and slide for maximum motion while maintaining contact and stability. The collateral ligaments provide side-to-side stability. The menisci increase the contact surface area between the round femoral condyles and the relatively flat tibial plateau on the medial side, and the convex tibial plateau on the lateral side and, therefore, play an important role in load transmission. When all or part of a meniscus is removed, the contact pressure between the femoral and tibial articular surfaces increases, which accelerates the wear and tear of articulating surfaces and seems to predispose to early arthrosis. Normal walking causes knee joint forces of 2 to 4 times body weight, 50% to 100% of which is transmitted through the meniscus. Patellofemoral joint forces vary with activity such as level walking, stair climbing or descending, deep knee bends and extension against resistance.
- Source: Robert C Schenck, Jr, MD, Editor: Athletic Training and Sports Medicine.
AAOS, Rosemont, IL, 1999.
Chapter 16: Knee Injuries, by Shelbourne KD, Rask BP and Hunt S.
Further Information:
- NIAMS: Questions and Answers About Knee Problems.
- LaPrade RF, Wentorf F. Acute Knee Injuries: On-the-Field and Sideline Evaluation. The Physician and Sportsmedicine, October 1999. Please note that free access to this article is no longer available.
- Bach BR. Acute Knee Injuries: When to Refer? The Physician and Sportsmedicine, May 1997. Please note that free access to this article is no longer available.
Page last updated on 29 January 2018
Site last updated on: 28 March 2014
|
 Disclaimer: This website is a source of information
and education resource for health professionals and individuals
with knee problems. Neither Chester Knee Clinic nor Vladimir Bobic
make any warranties or guarantees that the information contained
herein is accurate or complete, and are not responsible for
any errors or omissions therein, or for the results obtained from
the use of such information. Users of this information are encouraged
to confirm the accuracy and applicability thereof with other sources.
Not all knee conditions and treatment modalities are described
on this website. The opinions and methods of diagnosis and treatment
change inevitably and rapidly as new information becomes available,
and therefore the information in this website does not necessarily
represent the most current thoughts or methods. The content of
this website is provided for information only and is not intended
to be used for diagnosis or treatment or as a substitute for consultation
with your own doctor or a specialist. Email
addresses supplied are provided for basic enquiries and should
not be used for urgent or emergency requests, treatment of any
knee injuries or conditions or to transmit confidential or medical
information. If you have sustained a knee injury or have a medical condition,
you should promptly seek appropriate medical advice from your local
doctor. Any opinions or information,
unless otherwise stated, are those of Vladimir Bobic, and in no
way claim to represent the views of any other medical professionals
or institutions, including Nuffield Health and Spire Hospitals. Chester
Knee Clinic will not be liable for any direct, indirect,
consequential, special, exemplary, or other damages, loss or injury
to persons which may occur by the user's reliance on any statements,
information or advice contained in this website. Chester Knee Clinic is
not responsible for the content of external websites.
Disclaimer: This website is a source of information
and education resource for health professionals and individuals
with knee problems. Neither Chester Knee Clinic nor Vladimir Bobic
make any warranties or guarantees that the information contained
herein is accurate or complete, and are not responsible for
any errors or omissions therein, or for the results obtained from
the use of such information. Users of this information are encouraged
to confirm the accuracy and applicability thereof with other sources.
Not all knee conditions and treatment modalities are described
on this website. The opinions and methods of diagnosis and treatment
change inevitably and rapidly as new information becomes available,
and therefore the information in this website does not necessarily
represent the most current thoughts or methods. The content of
this website is provided for information only and is not intended
to be used for diagnosis or treatment or as a substitute for consultation
with your own doctor or a specialist. Email
addresses supplied are provided for basic enquiries and should
not be used for urgent or emergency requests, treatment of any
knee injuries or conditions or to transmit confidential or medical
information. If you have sustained a knee injury or have a medical condition,
you should promptly seek appropriate medical advice from your local
doctor. Any opinions or information,
unless otherwise stated, are those of Vladimir Bobic, and in no
way claim to represent the views of any other medical professionals
or institutions, including Nuffield Health and Spire Hospitals. Chester
Knee Clinic will not be liable for any direct, indirect,
consequential, special, exemplary, or other damages, loss or injury
to persons which may occur by the user's reliance on any statements,
information or advice contained in this website. Chester Knee Clinic is
not responsible for the content of external websites.
[ back to top ]